




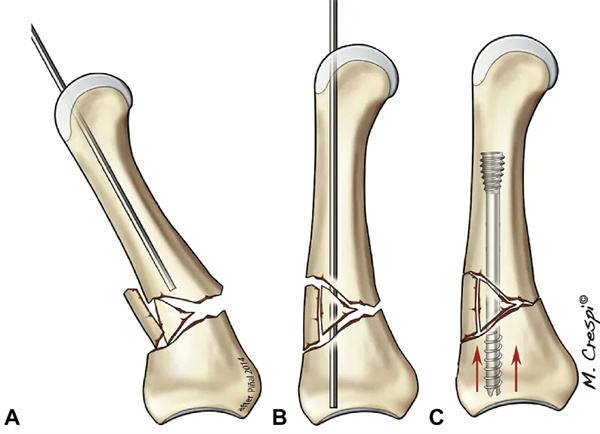
Karyewar da ta juye ba tare da wani abu ba ko kaɗan: idan aka sami karyewar ƙashin metacarpal (wuya ko diaphysis), a sake saita shi ta hanyar jan hankali da hannu. Ana lanƙwasa phalanx na kusa don fallasa kan metacarpal. An yi yanke mai zurfi na 0.5-1 cm kuma an ja jijiyar extensor a tsaye a tsakiyar layi. A ƙarƙashin jagorancin fluoroscopic, mun saka wayar jagora mai tsawon 1.0 mm tare da madaidaicin axis na wuyan hannu. An murƙushe ƙarshen wayar jagora don guje wa shigar cortical da kuma sauƙaƙe zamewa a cikin magudanar medullary. Bayan an tantance matsayin wayar jagora ta hanyar fluoroscopic, an sake gyara farantin ƙashin subchondral ta amfani da ɗan ramin haƙa rami kawai. An ƙididdige tsawon sukurori da ya dace daga hotunan kafin tiyata. A yawancin karyewar metacarpal, ban da metacarpal na biyar, muna amfani da sukurori mai diamita 3.0-mm. Mun yi amfani da sukurori marasa kai na AutoFIX (ƙananan Kashi Innovations, Morrisville, PA). Tsawon da za a iya amfani da shi na sukurori mai girman mm 3.0 shine mm 40. Wannan ya fi tsayin matsakaicin ƙashin metacarpal (kimanin cm 6.0), amma tsawonsa ya isa ya haɗa zaren a cikin medulla don samun madaidaicin sukurori. Diamita na ramin medullary na metacarpal na biyar yawanci babba ne, kuma a nan mun yi amfani da sukurori mai girman mm 4.0 tare da matsakaicin diamita har zuwa mm 50. A ƙarshen aikin, muna tabbatar da cewa an binne zaren caudal gaba ɗaya a ƙarƙashin layin cartilage. Akasin haka, yana da mahimmanci a guji dasa prosthesis sosai, musamman idan akwai karyewar wuya.
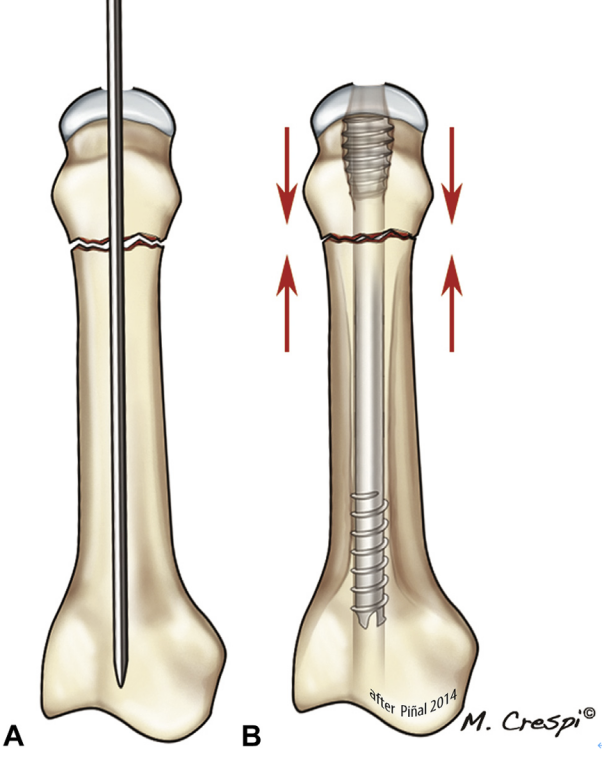
Hoto na 14 A cikin A, karyewar wuya ba ta da ƙarfi sosai kuma kan yana buƙatar ƙaramin zurfin jiki domin za a matse ɓangaren B.
Hanyar tiyata don karyewar phalanx mai wucewa ta hanyar phalanx mai kusanci ta yi kama da haka (Hoto na 15). Mun yi yanke mai wucewa ta 0.5 cm a kan phalanx mai kusanci yayin da muke lanƙwasa haɗin haɗin interphalangeal mai kusanci. An raba jijiyoyin kuma an ja su a tsayi don fallasa kan phalanx mai kusanci. Ga yawancin karyewar phalanx mai kusanci, muna amfani da sukurori mai 2.5 mm, amma ga manyan phalanges muna amfani da sukurori mai 3.0 mm. Matsakaicin tsawon CHS mai 2.5 mm da ake amfani da shi a yanzu shine 30 mm. Muna kula da kada mu ƙara matse sukurori. Tunda sukurori suna haƙa kansu kuma suna taɓa kansu, suna iya shiga tushen phalanx ba tare da juriya ba. An yi amfani da irin wannan dabarar don karyewar phalanx mai tsakiya, tare da yankewa yana farawa daga kan phalanx mai tsakiya don ba da damar sanya sukurori a baya.
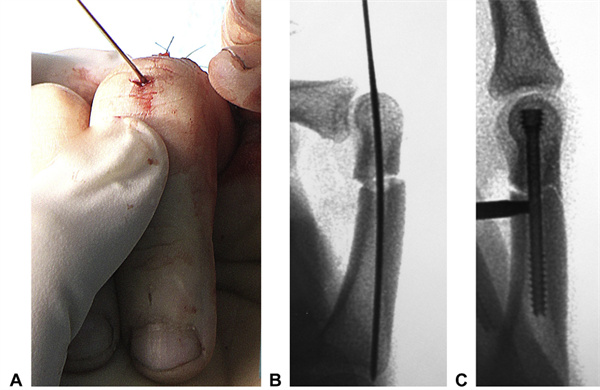
Hoto na 15. Duban cikin tiyata na akwati mai ratsa phalanx. An sanya wayar jagora ta AA mai 1-mm ta cikin ƙaramin yankewa mai ratsa tsaunin tare da madaidaicin phalanx na gaba.B An sanya wayar jagora don ba da damar daidaita wurin da aka sanya da kuma gyara duk wani juyawa. An saka CHS mai 2.5-mm CA kuma an binne shi a kai. Saboda takamaiman siffar phalanges, matsi na iya haifar da rabuwar metacarpal cortex. (Majiyyaci ɗaya kamar yadda yake a Hoto na 8)
Karyewar ƙashi: matsi mara tallafi yayin saka CHS na iya haifar da gajarta metacarpals da phalanges (Hoto na 16). Saboda haka, duk da cewa an haramta amfani da CHS a cikin irin waɗannan yanayi, mun sami mafita ga yanayi biyu da suka fi yawa da muke fuskanta.
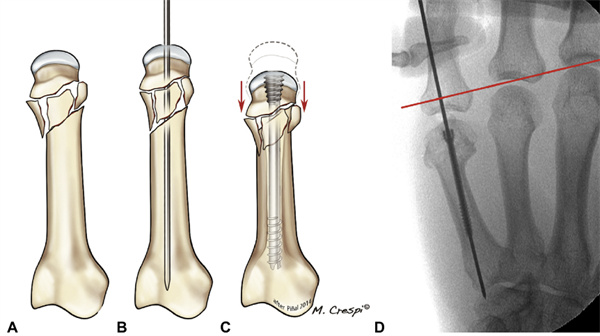
HOTO NA 16 AC Idan karyewar ba ta da alaƙa da cortical, matse sukurori zai haifar da rugujewar karyewar duk da raguwar gaba ɗaya. D Misalan da aka saba gani daga jerin marubutan sun yi daidai da lokutan raguwar matsakaicin (5 mm). Layin ja ya yi daidai da layin metacarpal.
Ga karaya ta submetacarpal, muna amfani da wata dabara da aka gyara bisa ga tsarin gine-gine na ƙarfafawa (watau, abubuwan gini da ake amfani da su don tallafawa ko ƙarfafa firam ta hanyar tsayayya da matsi na tsayi don haka suna tallafawa shi). Ta hanyar ƙirƙirar siffar Y tare da sukurori biyu, kan metacarpal ba ya rugujewa; mun sanya wa wannan takalmin takalmin siffar Y. Kamar yadda yake a cikin hanyar da ta gabata, ana saka wayar jagora mai tsayi 1.0 mm tare da ƙarshen ƙusa. Yayin da ake kiyaye madaidaicin tsawon metacarpal, ana saka wata wayar jagora, amma a kusurwa zuwa wayar jagora ta farko, don haka yana samar da tsari mai siffar triangle. An faɗaɗa wayoyi biyu na jagora ta amfani da madaidaicin karkatarwa don faɗaɗa medulla. Ga sukurori na axial da oblique, yawanci muna amfani da sukurori na diamita 3.0 mm da 2.5 mm, bi da bi. Da farko ana saka sukurori na axial har sai zaren caudal ya daidaita da guringuntsi. Sannan ana saka sukurori mai tsayi da ya dace. Tunda babu isasshen sarari a cikin magudanar medullary don sukurori guda biyu, ana buƙatar a ƙididdige tsawon sukurori masu kaifi a hankali, kuma ya kamata a haɗa sukurori masu kaifi a cikin sukurori masu kaifi kawai da zarar an binne su sosai a cikin kan metacarpal don tabbatar da isasshen kwanciyar hankali ba tare da fitowar sukurori ba. Sannan ana ci gaba da sukurori na farko har sai an binne shi gaba ɗaya. Wannan yana hana gajartar metacarpal a axial da rugujewar kai, wanda za a iya hana shi ta hanyar sukurori masu kaifi. Muna yin gwaje-gwajen fluoroscopic akai-akai don tabbatar da cewa rugujewar ba ta faru ba kuma sukurori suna da makulli a cikin magudanar medullary (Hoto na 17).
Hoto na 17 Fasahar AC Y-bracket
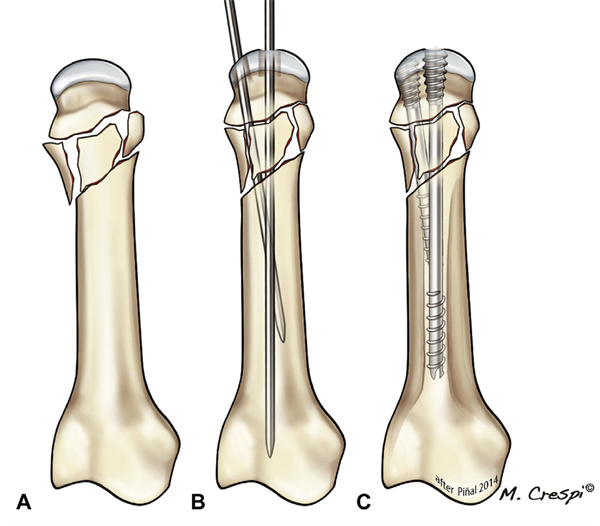
Lokacin da haɗin gwiwa ya shafi dorsal cortex a gindin proximal phalanx, mun ƙirƙiro wata hanyar da aka gyara; mun sanya masa suna bracing axial saboda sukurori yana aiki a matsayin katako a cikin phalanx. Bayan sake saita phalanx na proximal, an shigar da wayar jagora ta axial cikin medullary canal gwargwadon iyawa. Sannan ana saka CHS ɗan gajarta fiye da jimlar tsawon phalanx (2.5 ko 3.0 mm) har sai ƙarshen gabansa ya haɗu da farantin subchondral a gindin phalanx. A wannan lokacin, ana kulle zaren caudal na sukurori a cikin magudanar medullary, don haka suna aiki a matsayin tallafi na ciki da ƙarfafa tushen phalanx. Ana buƙatar gwaje-gwaje da yawa na fluoroscopic don hana shiga cikin haɗin gwiwa (Hoto na 18). Dangane da tsarin karyewa, ana iya buƙatar wasu sukurori ko haɗuwa da na'urorin gyara ciki (Hoto na 19).

Hoto na 19: Hanyoyi daban-daban na gyarawa ga marasa lafiya da suka ji rauni. Karya mai tsanani ta hanyar submetacarpal na yatsan zobe tare da gurɓataccen tushe na yatsan tsakiya (kibiya mai rawaya tana nuna yankin karyewar da aka yi).B An yi amfani da CHS na yau da kullun na 3.0 mm na yatsan manuniya, 3.0 mm paracentesis na yatsan tsakiya da aka yi amfani da shi, goyon bayan y na yatsan zobe (da dasa lahani a mataki ɗaya), da CHS na 4.0 mm na yatsan ruwan hoda.F An yi amfani da flaps masu kyauta don rufe nama mai laushi.C Radiography a cikin watanni 4. Kashin metacarpal na ƙaramin yatsan ya warke. Wasu ƙurajen ƙashi sun samo asali a wani wuri, suna nuna warkar da karyewar ta biyu.D Shekara ɗaya bayan hatsarin, an cire flap ɗin; kodayake ba shi da wata alama, an cire sukurori daga metacarpal na yatsan zobe saboda zargin shigar ciki cikin articular. An sami sakamako mai kyau (≥240° TAM) a kowane yatsa a ziyarar ƙarshe. Canje-canje a cikin haɗin gwiwar metacarpophalangeal na yatsan tsakiya sun bayyana a cikin watanni 18.
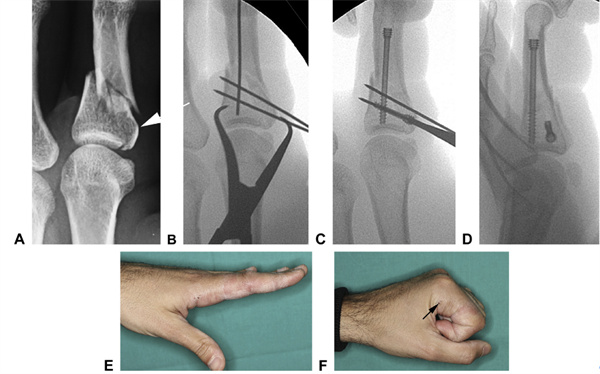
Hoto na 20 A Karyewar yatsan manuniya tare da tsawaitawa ta cikin jijiyoyin jini (wanda aka nuna ta hanyar kibiyoyi), wanda aka canza zuwa karaya mai sauƙi ta hanyar gyara karyewar haɗin gwiwa na ɗan lokaci ta amfani da waya ta K.C Wannan ya ƙirƙiri tushe mai ƙarfi wanda aka saka sukurori mai tallafi na tsayi.D Bayan gyarawa, an yi la'akari da cewa ginin yana da ƙarfi, yana ba da damar motsi nan take.E,F. Tsawon motsi a makonni 3 (kibiyoyi suna nuna wuraren shiga sukurori na asali)
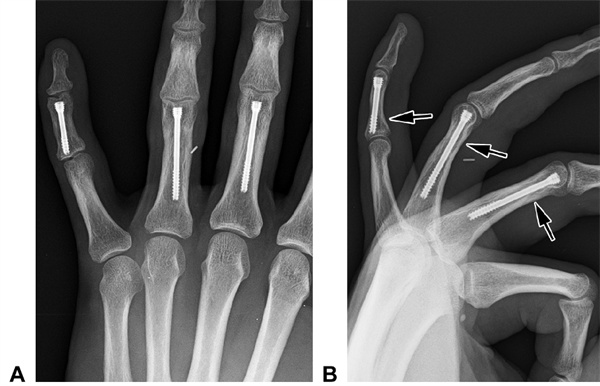
Hoto na 21 Hotunan rediyo na baya na orthostatic da B na gefe na majiyyaci A. An yi wa majiyyacin magani da sukurori masu girman 2.5-mm na cannulable. Babu wani muhimmin canji a cikin haɗin gwiwar interphalangeal da aka gani bayan shekaru 2.
Lokacin Saƙo: Satumba-18-2024





